Share
Over the last several years Minimally Invasive Glaucoma Surgery (MIGS) devices have become important parts of an ophthalmologist’s armamentarium.
These devices provide the means by which aqueous can bypass areas of outflow limitation with less tissue manipulation and fewer severe complications than traditional trabeculectomy. Due to these perceived benefits, general ophthalmologists and glaucoma subspecialists are increasingly making use of MIGS.
This prompts one to ask: Is trabeculectomy now completely outdated?
There are a number of reasons why trabeculectomy has long been considered the gold standard for the treatment of uncontrolled glaucoma. Primarily, it has produced effective, long-term results. One of the longest-term studies shows an 88% qualified success rate, even after 20 years. In comparison, few MIGS studies have extended beyond 36 months.
Trabeculectomy is also highly effective at lowering eye pressure. In the most recent studies comparing trabeculectomy to tube shunt implantation, trabeculectomy has ultimately resulted in lower levels of intraocular pressure (IOP). For patients with advanced glaucoma requiring low eye pressure targets, trabeculectomy is often required.
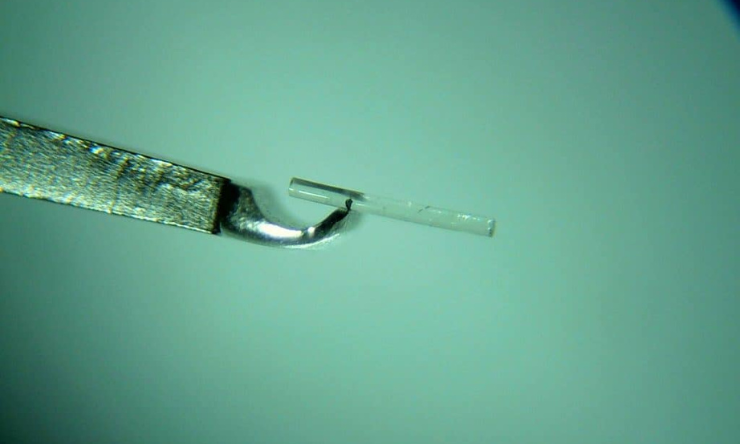
Secondly, trabeculectomy does not require a specially designed device. MIGS devices increase surgical expense and are not without the risk of complications. For example, some degree of hyphaema is not uncommon in MIGS procedures, and cases of stent erosion and endophthalmitis have also been reported for the XEN stent.
Furthermore, following the recall of the CyPass suprachoroidal stent due to concerns of its long-term effect on corneal endothelial cells, questions are being raised regarding the long-term safety of MIGS devices.
The emergence of MIGS also raises a secondary issue over doctors maintaining their operative proficiency. If trabeculectomies are performed less frequently, ophthalmologists could become deskilled in this area.
Australia is an important training centre for international fellows. In developing countries where cost limits the availability of MIGS, trabeculectomy will remain a critical procedure for some time. Therefore, trabeculectomies remain important in Australia to ensure skills are maintained and training is available to those who need it.
Despite these challenges, it is not difficult to understand why MIGS has increased in popularity. Prior to its introduction there was no intermediary step between Selective Laser Trabeculoplasty (SLT) and glaucoma filtration surgery. Most ophthalmologists who regularly perform trabeculectomies understand the complexity and extensive follow up required to manage outcomes.
For instance, studies have reported a five-year reoperation rate of 25% for trabeculectomy. The technical demand required to prevent and manage complications has seen trabeculectomy increasingly being performed by ophthalmologists with glaucoma subspecialist training.
MIGS has provided a bridge between medication or laser treatment and glaucoma filtration surgery. On one side, ophthalmologists are increasingly utilising trans-trabecular stents at time of cataract surgery for glaucoma patients with inadequately controlled IOP or an intolerance to eye drops. On the other, the XEN filtration stent is being adopted by more ophthalmologists with glaucoma subspecialist interest as an alternative to trabeculecotmy with reduced risks.
Importantly, MIGS have also prompted an evolution of the surgical approach to glaucoma. This will see future incremental improvements to MIGS devices, making them safer and more effective. The recent Medical Research Futures Fund directed to the development of Australian medical devices might stimulate further progress in this area.
In summary, MIGS devices have given ophthalmologists an increased range of options for treating glaucoma, but it is far too soon to consider trabeculectomy an obsolete procedure. Both procedures will still have their place in an ophthalmologist’s toolbox for some time. Although, current trends and advances in MIGS could change this in the not too distant future.
Subscribe to our FREE Glaucoma Australia eNewsletter Here: glaucoma.org.au/news/subscribe-to-glaucoma-enews/


During the past decade, glaucoma care in the UK has changed dramatically, with more non-medical ophthalmic practitioners involved. As such, optometrists and other non-medical professionals have been delivering laser treatments including SLT in the Hospital Eye Service (HES).
Sustained drug delivery via an implant could reduce the reliance on daily eye drops and ensure that the correct amount of medicine is delivered consistently, every day.
With the rising numbers of patients diagnosed with glaucoma – and oversubscription of public ophthalmology departments – the Glaucoma Community Collaborative Care Program at the Royal Victorian Eye and Ear Hospital in Melbourne is designed to alleviate some of this pressure.