Share
Glaucoma is the leading cause of irreversible blindness worldwide. Intraocular pressure (IOP) control is the most important factor in preventing glaucoma progression. In patients with mild to moderate glaucoma, minimally invasive glaucoma surgery (MIGS) has emerged as a promising new treatment option.

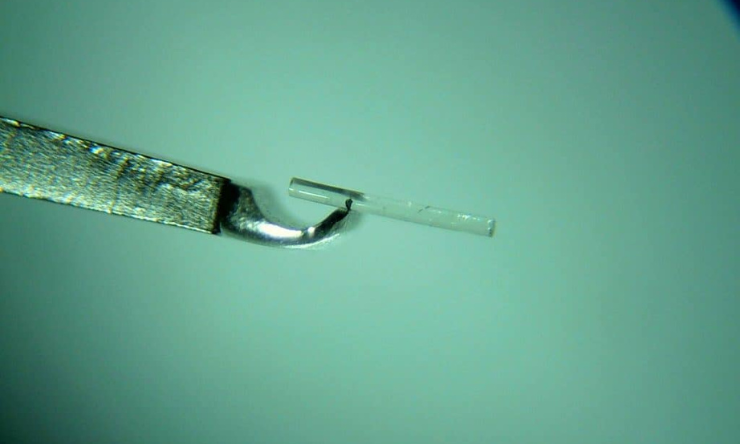
The iStent is a small medical device inserted into the eye to increase the amount of fluid drainage to lower eye pressures. Research has been conducted to determine if cataract surgery, in combination with glaucoma surgery, could be more successful in lowering eye pressures in people with Primary Angle Closure Glaucoma (PACG) than having cataracts surgery alone.
Drainage angles are narrow in primary angle closure glaucoma which results in less fluid being able to leave the eye resulting in higher eye pressures. By removing the cataract which widens the drainage angles, and by placing a drainage device in the eye to allow more fluid to leave the eye, a greater reduction in eye pressure can be achieved.
The study concluded, iStent implantation in combination with cataract surgery resulted in significantly higher rates of complete success compared with cataracts surgery alone - with a higher proportion of angle closure eyes not requiring glaucoma medications after the surgery.
In view of the potentially sight‐threatening complications, most surgeons are reluctant to perform combined surgeries in patients with medically controlled glaucoma. However, the study showed that combined Phaco‐iStent (cataracts surgery and iStent) has a favourable safety profile, and the incidence of complications was comparable with cataracts surgery alone; and no sight‐threatening complications were reported.
Reference
Chen D. Z et al. 2020, Phacoemulsification vs phacoemulsification with micro‐bypass stent implantation in primary angle closure and primary angle closure glaucoma: A randomized single‐masked clinical study, Clinical and Experimental Ophthalmology, Volume 48, Issue 4, pp. 450-461, RANZCO
< https://doi-org.ezproxy.lib.swin.edu.au/10.1111/ceo.13721>

During the past decade, glaucoma care in the UK has changed dramatically, with more non-medical ophthalmic practitioners involved. As such, optometrists and other non-medical professionals have been delivering laser treatments including SLT in the Hospital Eye Service (HES).
Sustained drug delivery via an implant could reduce the reliance on daily eye drops and ensure that the correct amount of medicine is delivered consistently, every day.
With the rising numbers of patients diagnosed with glaucoma – and oversubscription of public ophthalmology departments – the Glaucoma Community Collaborative Care Program at the Royal Victorian Eye and Ear Hospital in Melbourne is designed to alleviate some of this pressure.